Patella Instability
Patella (Kneecap) Instability
Patella instability — where the kneecap slips out of place or dislocates — can be addressed with targeted soft-tissue and bony procedures to restore stable, confident movement.
Key points
- Recurrent kneecap dislocation or subluxation
- Rotational profile assessment
- MPFL (medial patellofemoral ligament) reconstruction
- Tibial Tubercle Osteotomy (TTO) for malalignment
- Combined procedures where indicated
- Tailored to your anatomy, activity level and goals
Physiotherapy first
Before considering surgery, a structured physiotherapy programme is essential. The muscles around the hip and thigh — particularly the quadriceps, hip abductors and external rotators — play a critical role in controlling kneecap position and preventing dislocation.
Targeted exercises that strengthen the vastus medialis obliquus (VMO), improve hip control and correct movement patterns can significantly reduce episodes of instability in many patients. Gait retraining, proprioceptive work and taping or bracing may also form part of the initial management.
The evidence supports this approach. Studies have shown that conservative treatment with physiotherapy can achieve good results in first-time dislocators and in patients with milder instability. Even when surgery is ultimately required, preoperative physiotherapy improves muscle tone, range of movement and postoperative recovery. I always recommend a dedicated trial of physiotherapy before deciding on operative intervention.
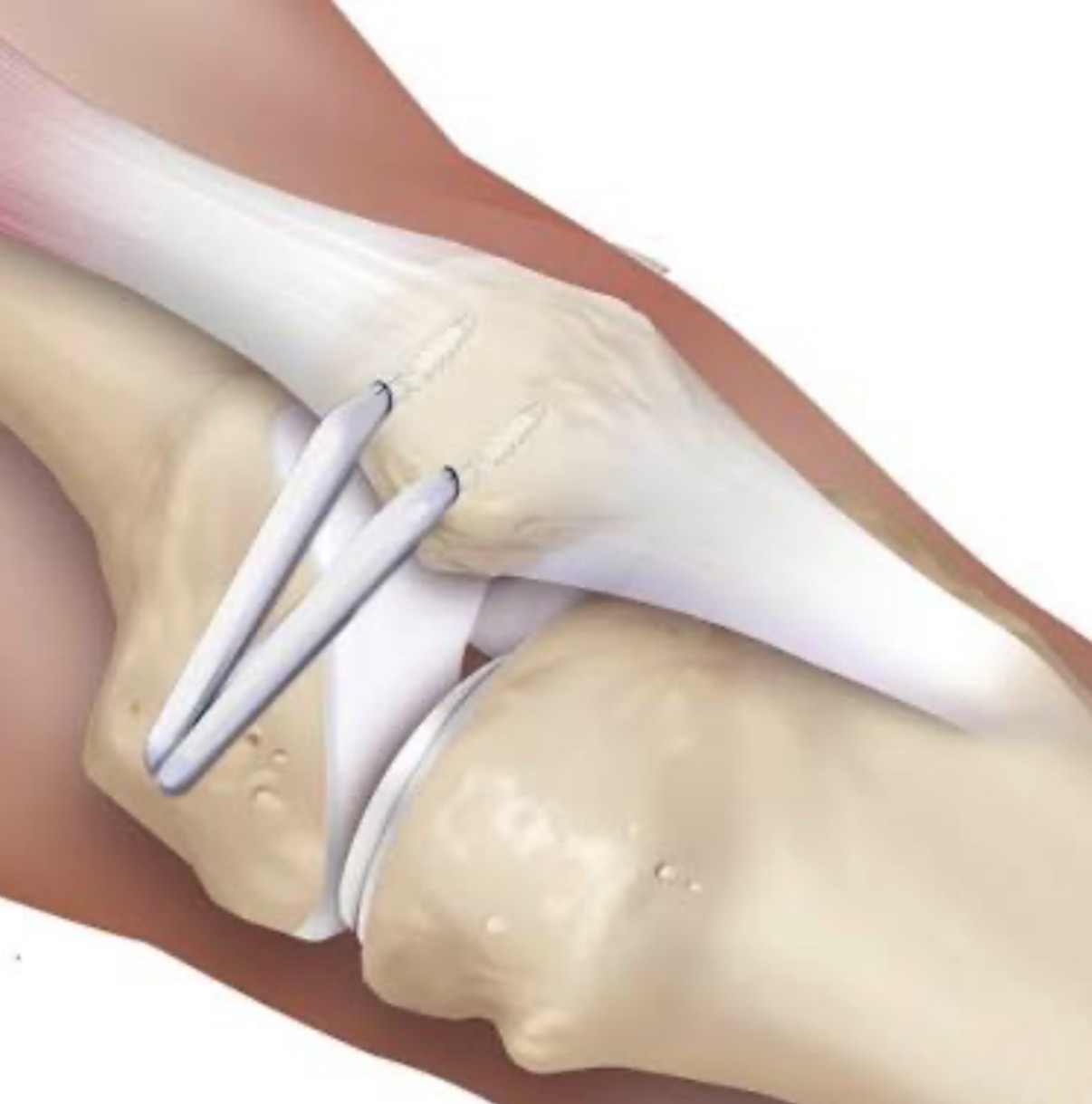
The MPFL and recurrent dislocation
The medial patellofemoral ligament (MPFL) is the primary restraint that stops the kneecap from dislocating toward the outside of the knee. It is a strong band of tissue that tethers the inner edge of the patella to the inner side of the femur, acting like a check-rein that holds the kneecap within its groove.
When the kneecap dislocates for the first time — usually with a twisting injury or direct blow — the MPFL is almost always torn or stretched. This is the critical event that changes the knee from a stable joint to one that is prone to further episodes. Without a functioning MPFL, the patella has no reliable soft-tissue brake against lateral displacement, and the risk of recurrent dislocation rises dramatically.
Why this matters: once the MPFL has been damaged, the patella becomes free to slip or dislocate with far less force. Simple activities such as getting out of a car, turning in bed, or stepping off a curb can trigger another episode. Repeated dislocations cause further damage to the articular cartilage on the back of the patella and the edge of the femoral groove, which can lead to arthritis over time.
This is why I place such importance on identifying MPFL injury early. In patients with recurrent instability, the torn or attenuated MPFL is the key structural problem that must be addressed — whether through careful rehabilitation in select cases, or through reconstruction when the ligament has failed to heal and instability persists.
Other factors that contribute to patellar instability
While the MPFL is the primary soft-tissue restraint, several anatomical factors work together to make dislocation more likely. Understanding these is essential when planning treatment, because correcting the MPFL alone may not be enough if the underlying bony architecture leaves the patella vulnerable.
Patella alta — a high-riding kneecap — means the patella does not sit deep enough within the trochlear groove of the femur. In early flexion, when the knee begins to bend, the patella is essentially sitting above the groove rather than within it. This leaves it free to slide sideways with little resistance, and is one of the strongest predictors of recurrent dislocation. Normalising patellar height through distalisation at the time of surgery is often a key part of achieving long-term stability.
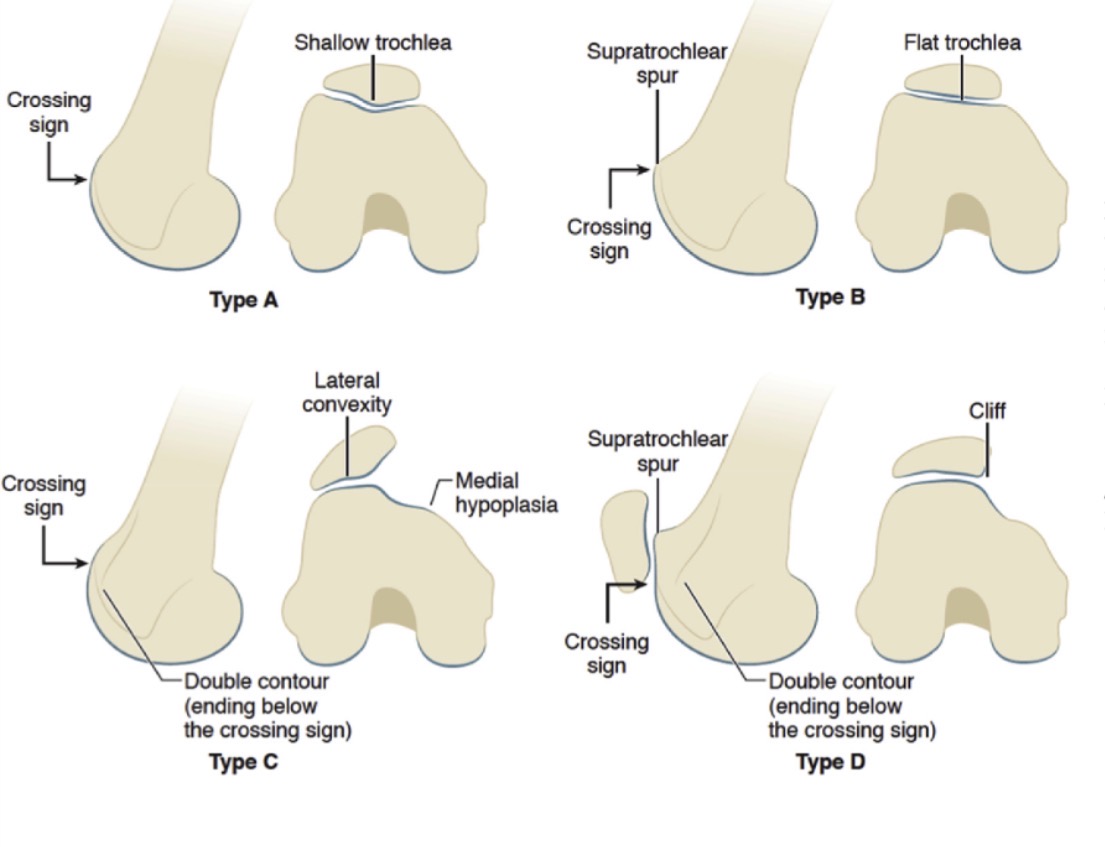
Trochlear dysplasia refers to an abnormally shallow or flat groove at the end of the femur where the kneecap should track. In a normal knee, the bony walls of the trochlear groove rise up on either side and guide the patella as the knee bends. When these walls are underdeveloped or flattened, there is nothing to hold the kneecap in place. Trochlear dysplasia is a powerful risk factor for instability and, in severe cases, may require deepening the groove (trochleoplasty) as part of a comprehensive stabilisation procedure.
Tight lateral structures — including the lateral retinaculum and iliotibial band — can pull the kneecap persistently toward the outside of the knee. When these structures are too tight, they create a constant lateralising force that the weakened or torn MPFL cannot counteract. Releasing these tight structures (lateral release) during MPFL reconstruction restores a more balanced force environment around the patella and improves tracking.
Rotational malalignment of the femur and tibia is an often-overlooked contributor. When the thigh bone is excessively rotated inward (increased femoral anteversion) or the shin bone is rotated outward (external tibial torsion), the entire mechanical axis of the leg changes. This alters the line of pull of the quadriceps and patellar tendon, directing force laterally across the patellofemoral joint with every step. These rotational abnormalities are assessed on specialised imaging and may influence whether a tibial tubercle osteotomy or even a derotational osteotomy is needed alongside soft-tissue reconstruction.
These factors rarely exist in isolation. A patient with trochlear dysplasia may also have patella alta and a torn MPFL — the so-called "miserable malalignment" pattern. This is why a thorough assessment of all contributing elements is essential, and why treatment must be individualised to address not just the torn ligament, but the entire structural environment that allowed the dislocation to occur in the first place.
Why Tibial Tubercle Osteotomy helps — especially in patella alta
Patella alta — a high-riding kneecap — is one of the most important risk factors for recurrent patellar dislocation. When the patella sits too high, it does not engage properly in the trochlear groove at the front of the femur, leaving it vulnerable to slipping sideways, particularly in early knee flexion.
A TTO addresses this by moving the attachment point of the patellar tendon on the tibia. In patella alta, the key manoeuvre is distalisation — moving the tibial tubercle downwards (distally). This effectively lowers the patella into a better position within the trochlear groove, improving both stability and patellar tracking throughout the range of movement.
Distalisation works by lengthening the lever arm of the extensor mechanism and increasing the contact area between the patella and the femur. By normalising patellar height, the kneecap engages the bony walls of the trochlea earlier as the knee bends, which provides far greater resistance to lateral displacement. This is especially valuable in patients who have failed previous soft-tissue surgery or who have severe patella alta on imaging.
The procedure can also be combined with medialisation (moving the tubercle inward) when there is increased TT-TG distance or rotational malalignment, allowing a truly individualised correction based on each patient's anatomy.
Surgery and rehab for MPFL reconstruction
0 – 6 weeks
- Full weight bearing on crutches
- Physiotherapy
6 weeks – 3 months
- Quadriceps strengthening
MPFL Reconstruction and TTO
0 – 2 months
- Crutches
- Physiotherapy
- Brace keeping leg straight when weight bearing
- Bending allowed when not weight bearing
2 months – 4 months
- If TTT united, remove brace and full rehab
Valgus alignment of the leg
Valgus describes a knock-kneed posture where the lower leg angles outward relative to the thigh, so that the knees come together or even touch when the ankles are kept apart. This alters the line of pull of the quadriceps and patellar tendon, increasing the lateralising forces on the kneecap and making dislocation more likely.
Significant valgus malalignment is an important but sometimes overlooked contributor to patellar instability. When the mechanical axis of the leg falls medial to the knee centre, the patella is effectively pulled laterally with every step and squat. In these cases, a distal femoral osteotomy (DFO) may be discussed to correct the coronal plane alignment, realign the extensor mechanism and protect the patellofemoral joint.
DFO for patella stabilization
- Realigns the mechanical pull of the kneecap by correcting coronal plane valgus
- Reduces lateralising forces on the patella with every step and squat
- Protects the patellofemoral joint from recurrent dislocation and long-term wear
- Restores a neutral mechanical axis so the extensor mechanism tracks correctly
Surgery
- Usually one night stay in hospital to help control pain
- Lots of local anaesthetic will be given at the time of surgery
Rehab
- Usually full weight bearing from day one as pain allows
- If combined with a TTO (above) then will be bespoke and individual to each patient
0 – 6 weeks
- On crutches
- Physiotherapy
- Partially or fully weight bearing (with or without a brace)
- Full range of movement of your knee
6 weeks – 12 weeks
- Definitely fully weight bearing
- Repeat X-ray to ensure osteotomy healing
12 weeks – 6 months
- Improve with strength and activities
18 months
- Remove plate
Important points after surgery
- Driving: Not insured for 6 weeks minimum from the date of surgery.
- Flying: Advise not to fly for 3 months after surgery due to increased risk of blood clots.
After surgery if you or anyone have concerns about your wound please contact my secretary or myself and do not start any antibiotics unless advised by myself.