Treatments
Meniscal Tears
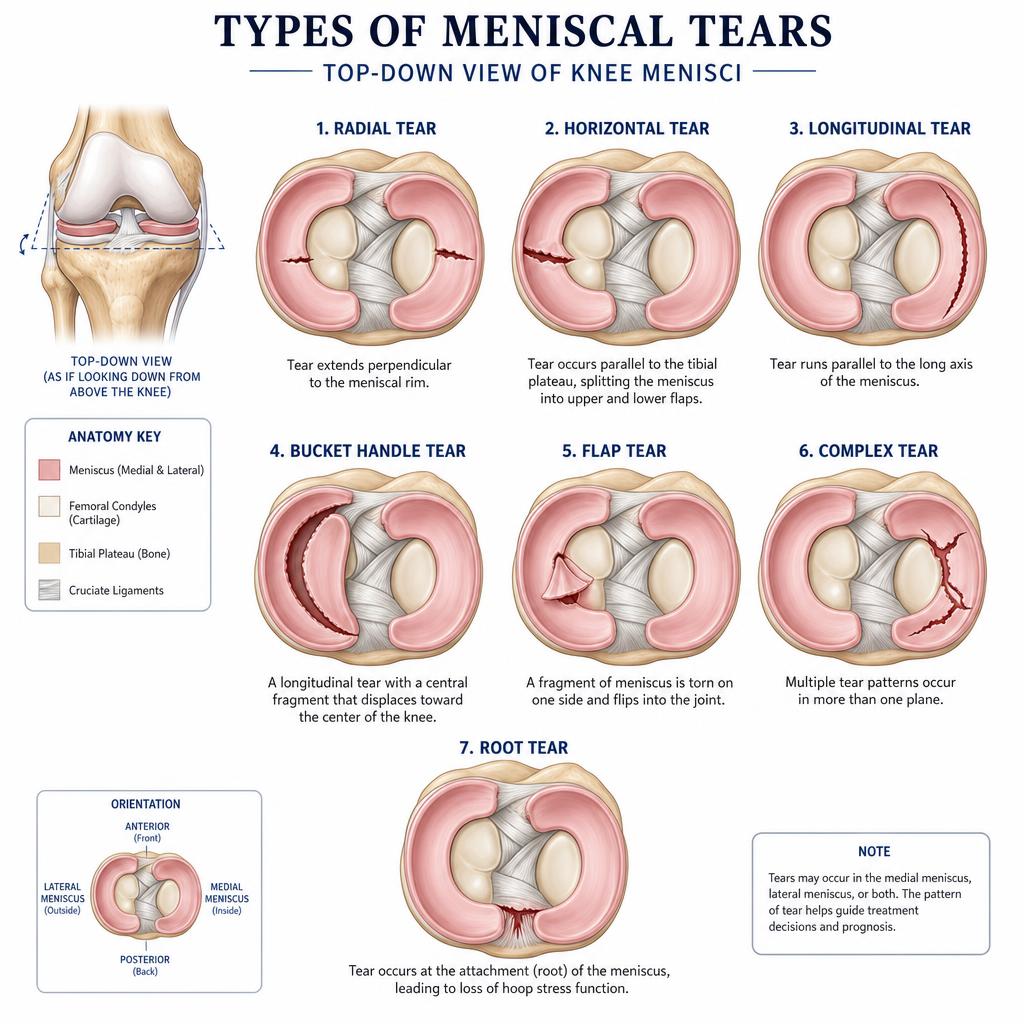
The meniscus is a C-shaped shock absorber inside the knee. Tears are one of the most common knee injuries and the right treatment depends on your age, activity level, the pattern of the tear, and whether arthritis is also present.
Active patients · no arthritis
Tears in active patients with no arthritis
In younger, active patients with a healthy knee and no underlying arthritis, a meniscal tear is usually the result of a twisting injury during sport or daily activity. Symptoms typically include pain along the joint line, swelling, catching, and sometimes locking of the knee.
My approach is always preservation-first. Wherever the tear pattern allows, I will repair the meniscus rather than remove it. Preserving meniscal tissue protects the articular cartilage and significantly reduces the long-term risk of developing arthritis. Repair is performed arthroscopically as daycase surgery, followed by a structured rehabilitation programme to protect the repair while restoring strength and movement.
When a tear is not suitable for repair, only the damaged portion is carefully trimmed (partial meniscectomy), leaving as much healthy meniscus as possible.

Meniscal tears with arthritis
Treatment when arthritis is also present
In patients with established arthritis, a meniscal tear is often part of the wider wear pattern in the joint rather than the sole cause of pain. Arthroscopic surgery for a degenerate meniscal tear in an arthritic knee does not reliably relieve symptoms and is not usually recommended.
Instead, treatment focuses on managing the arthritis itself. This may include physiotherapy and muscle strengthening, weight management, activity modification, simple analgesia, and intra-articular injections such as steroid, hyaluronic acid, Arthrosamid, PRP or BMAC. Where arthritis is more advanced and conservative measures are no longer effective, realignment surgery (osteotomy), partial knee replacement or total knee replacement may be considered depending on the pattern and severity of joint involvement.
NB: personally I don't recommend or give steroid injections for knees except in exceptional circumstances.
Urgent · bucket handle tears
Bucket handle meniscal tears
A bucket handle tear is a large longitudinal tear where a fragment of the meniscus displaces into the centre of the joint, often blocking the knee from fully straightening. This presents as a locked knee, with a clear mechanical block to full extension, pain, and swelling.
Bucket handle tears are urgent. The displaced fragment should be reduced and repaired as soon as possible — ideally within a few weeks — because the meniscal tissue is at its most repairable while it is still healthy, well-vascularised and undeformed. Delays reduce the chance of a successful repair and increase the risk of needing to remove the fragment instead, which has long-term consequences for the joint.
If you have a locked knee or suspect a bucket handle tear, please seek urgent assessment so that imaging and surgery can be arranged promptly.
Surgery
I always attempt to repair bucket handle tears utilizing different techniques. Depending how quickly you present, are diagnosed and get to theatre will be one factor determining whether your tear is repairable or not.
Rehabilitation
0 – 6 weeks
NWB with crutches
Non weight bearing with crutches. You will be placed in a brace and allowed to bend from 0–90 degrees.
6 – 12 weeks
Full weight bearing
Full weight bearing, remove brace and continue physiotherapy.
3 – 6 months
Return to normal
Continue with strength training of thigh muscles and return to normal.
Meniscal root tears
Meniscal root tears
A meniscal root tear is a tear at the point where the meniscus attaches firmly to the tibia. Functionally, a root tear behaves like a complete loss of the meniscus, because the meniscus can no longer convert load into hoop stresses and protect the cartilage. Untreated, root tears are strongly associated with rapid progression of arthritis and, in some cases, subchondral insufficiency fractures.
Patients often describe a sudden pop at the back of the knee, sometimes during a deep squat or a relatively minor movement, followed by significant pain and swelling. MRI is essential to confirm the diagnosis.
In suitable patients — particularly those who are active, have minimal or no arthritis, and present early — I recommend arthroscopic meniscal root repair. The torn root is re-attached to its anatomical footprint on the tibia using transtibial sutures, restoring the meniscus's protective function. Early diagnosis and timely surgery give the best chance of preserving the joint and avoiding accelerated arthritis.
Surgery
Surgery for these repairs is different. I will assess and see if it is repairable. If it is I will drill a narrow tunnel in your tibia and pull the stitches I place in your meniscal root through this tunnel and tie it at the front of your tibia (shin bone) under the skin.
Rehabilitation
0 – 6 weeks
NWB with crutches
Non weight bearing with crutches. You will be placed in a brace and allowed to bend from 0–90 degrees.
6 – 12 weeks
Full weight bearing
Full weight bearing, remove brace and continue physiotherapy.
3 – 6 months
Return to normal
Continue with strength training of thigh muscles and return to normal.
Ramp lesions
Meniscal ramp lesions
A ramp lesion is a longitudinal tear of the meniscus at its peripheral attachment at the back of the knee, where the meniscus meets the capsule. It is often associated with ACL injuries and can easily be missed on standard MRI views or during routine arthroscopy if the posterior aspect of the joint is not carefully inspected.
Because these tears sit at the very back of the knee, they can be difficult to see and access through the standard two arthroscopy portals. I use a third portal — the posteromedial portal — which gives a direct view and working access to the posterior horn of the meniscus, allowing the tear to be identified and repaired more easily and reliably.
Surgery
The ramp lesion is repaired arthroscopically using sutures to reattach the meniscus to the capsule. By adding the posteromedial portal I can place stitches accurately under direct vision, giving the repair the best chance of healing.
Rehabilitation
0 – 6 weeks
NWB with crutches
Non weight bearing with crutches. You will be placed in a brace and allowed to bend from 0–90 degrees.
6 – 12 weeks
Full weight bearing
Full weight bearing, remove brace and continue physiotherapy.
3 – 6 months
Return to normal
Continue with strength training of thigh muscles and return to normal.
Meniscal allograft transplants
Meniscal Allograft Transplants (MAT)
- Significant pain on the affected side
- Previous surgery which removed a large amount of meniscal tissue
- No severe arthritis present
- May be combined with a knee osteotomy (HTO/DFO) to protect transplanted tissue (see realignment page)
- Usually performed in specific centres as relatively rare
A meniscal allograft transplant (MAT) is a procedure where a donor meniscus is used to replace a meniscus that has been previously removed or is irreparably damaged. The transplanted meniscus restores the shock-absorbing function of the knee, redistributes load across the joint, and helps protect the articular cartilage from further wear.
MAT is considered in younger, active patients who have had a previous meniscectomy and are experiencing ongoing pain, swelling, or early signs of cartilage wear because the meniscus is no longer there to protect the joint. It is not suitable for patients with established arthritis, as the procedure requires a relatively healthy cartilage surface to give the transplant the best chance of success.
Careful patient selection is essential. The size and shape of the donor meniscus must be matched closely to the patient's own, and the alignment and stability of the knee must be assessed beforehand. When these conditions are met, MAT can provide significant pain relief and help delay or avoid the need for joint replacement surgery.
If a meniscal allograft transplant is indicated, I would refer you to a colleague who specialises in this surgery so that you receive the very best care from a surgeon who performs this procedure regularly.
Informed consent
Risks of meniscal surgery
All surgery carries risks. For meniscal repair and meniscectomy, these include:
- Infection — a small risk with any arthroscopic procedure, usually treatable with antibiotics.
- Bleeding — generally minimal, but can occasionally require drainage or transfusion.
- Common peroneal nerve injury — with lateral meniscal repairs causing foot drop and loss or altered sensation over outside of leg below your knee and top of your foot.
- Further surgery — the repair may fail to heal or symptoms may persist, requiring a second procedure.
- Inability to repair — at the time of surgery the meniscal damage may be greater than expected, making repair impossible and requiring partial removal instead.
- Post-traumatic arthritis acceleration — loss of meniscal tissue increases load on the cartilage and can speed up the development of arthritis over time.
- Scars — small portal scars are usually minimal, but can occasionally be more prominent or cause discomfort.